Autar DVT Scale
The Autar DVT scale is composed of seven risk categories; increasing age, build and body mass index (BMI), immobility, special DVT risk, trauma, surgery, and high risk disease. Each category or risk factor is scored on a 0-4 scale.
Score Type of Risk
0-1 No or Little Risk
2-3 Low to Moderate Risk
>4 High Risk
After each of the seven risk categories are assessed the scores are totaled and the assessment protocol is used to determine if the patient is at risk of acquiring a DVT.
Assessment Protocol
Score Type of Risk
<6 No Risk
7-10 Low Risk (<10%)
11-14 Moderate Risk (11-40%)
>15 High Risk (>41%)
Validity of the Autar DVT Scale
Sensitivity Specificity
100% 81%
The Autar DVT scale is composed of seven risk categories; increasing age, build and body mass index (BMI), immobility, special DVT risk, trauma, surgery, and high risk disease. Each category or risk factor is scored on a 0-4 scale.
Score Type of Risk
0-1 No or Little Risk
2-3 Low to Moderate Risk
>4 High Risk
After each of the seven risk categories are assessed the scores are totaled and the assessment protocol is used to determine if the patient is at risk of acquiring a DVT.
Assessment Protocol
Score Type of Risk
<6 No Risk
7-10 Low Risk (<10%)
11-14 Moderate Risk (11-40%)
>15 High Risk (>41%)
Validity of the Autar DVT Scale
Sensitivity Specificity
100% 81%
| Autar DVT Risk Assessment Scale |
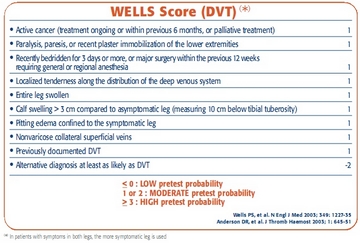
Wells' Clinical Decision Rule for DVT (VIDEO)
Scoring
High DVT Risk = score of 3+ (75% Probability for DVT)
According to Wells' CDR, patients who are high risk for DVT should be referred for ultrasound test first. If test is positive, rule in DVT. If test is negative, the patient is referred for another ultrasound test approximately one week later. If that test is negative, rule out DVT. If the test is positive, rule in DVT.
Moderate DVT Risk = score of 1-2 (17% Probability for DVT)
According to Wells' CDR, patients who are moderate risk for DVT should be referred for ultrasound test first. If the test is positive, rule in DVT. If the ultrasound is negative, a D-dimer blood test (looks for protein fragment in the blood from clot breakdown) is warranted. If the D-dimer is negative, rule out DVT. If the blood test comes back positive, the patient again is referred for ultrasound approximately one week later. If the test is negative, rule out DVT. If the test is positive, rule in DVT.
Low DVT Risk = score of < 1 (3% Probability for DVT)
According to Wells' CDR, patients who are low risk for DVT should be referred for a D-Dimer blood test. If the D-Dimer comes back negative rule out DVT. If the blood test comes back positive, an ultrasound test is warranted. If ultrasound comes back negative, rule out DVT. If it comes back positive, rule in DVT.
Wells CDR validation Since 1995...
Study Sensitivity Specificity
Sohne 2005 100% 45%
Aguillar 2006 100% 30%
Schutgens 2006 100% 35%
Carrier 2008 96% 70%
Scoring
High DVT Risk = score of 3+ (75% Probability for DVT)
According to Wells' CDR, patients who are high risk for DVT should be referred for ultrasound test first. If test is positive, rule in DVT. If test is negative, the patient is referred for another ultrasound test approximately one week later. If that test is negative, rule out DVT. If the test is positive, rule in DVT.
Moderate DVT Risk = score of 1-2 (17% Probability for DVT)
According to Wells' CDR, patients who are moderate risk for DVT should be referred for ultrasound test first. If the test is positive, rule in DVT. If the ultrasound is negative, a D-dimer blood test (looks for protein fragment in the blood from clot breakdown) is warranted. If the D-dimer is negative, rule out DVT. If the blood test comes back positive, the patient again is referred for ultrasound approximately one week later. If the test is negative, rule out DVT. If the test is positive, rule in DVT.
Low DVT Risk = score of < 1 (3% Probability for DVT)
According to Wells' CDR, patients who are low risk for DVT should be referred for a D-Dimer blood test. If the D-Dimer comes back negative rule out DVT. If the blood test comes back positive, an ultrasound test is warranted. If ultrasound comes back negative, rule out DVT. If it comes back positive, rule in DVT.
Wells CDR validation Since 1995...
Study Sensitivity Specificity
Sohne 2005 100% 45%
Aguillar 2006 100% 30%
Schutgens 2006 100% 35%
Carrier 2008 96% 70%
| wells_clinical_decision_rule_for_dvt.jpg |
Ultrasound Imaging
Ultrasound Imaging is considered to be the first-choice diagnostic test for patients in the moderate- to high-probability groups for DVT. To perform compression ultrasound a 3- to 7.5-MHz transducer is used to produce an image of the suspected vein. To perform this procedure in the lower extremity the patient is positioned in supine with his/her lower extremity externally rotated. The transducer is applied to the skin with enough compression to indent the skin but does not compromise the arterial blood supply. Testing starts at the inguinal region and is moved distally down to the calf. When the vein that is being examined is not collapsible the test is determined to be positive.
Accuracy of Ultrasonography
Study Sensitivity Specificity
Wells 1995 78% 98%
Ultrasound Imaging is considered to be the first-choice diagnostic test for patients in the moderate- to high-probability groups for DVT. To perform compression ultrasound a 3- to 7.5-MHz transducer is used to produce an image of the suspected vein. To perform this procedure in the lower extremity the patient is positioned in supine with his/her lower extremity externally rotated. The transducer is applied to the skin with enough compression to indent the skin but does not compromise the arterial blood supply. Testing starts at the inguinal region and is moved distally down to the calf. When the vein that is being examined is not collapsible the test is determined to be positive.
Accuracy of Ultrasonography
Study Sensitivity Specificity
Wells 1995 78% 98%
Homan's Sign (VIDEO)
Homan's sign is used by many clinicians as evidence of DVTs but IS NOT specific or sensitive (around 50%) for DVT because a positive Homan's sign is possible with Achilles tendinitis and muscle injury of the gastrocnemius and plantar muscle. This test has been shown to be an "unreliable test for DVT." The test is done by using slow dorsiflexion of the foot, knee extension, or gentle squeezing/deep palpation of the affected calf to elicit deep calf pain because "in theory, the inflamed nerves in the veins within the muscle are compressed or stretched causing deep calf pain. One main reason this test is unreliable is that only "about half of all clients with DVT experience pain and Homan's sign" (Goodman and Snyder & O'Sullivan and Schmitz).
Homan's sign is used by many clinicians as evidence of DVTs but IS NOT specific or sensitive (around 50%) for DVT because a positive Homan's sign is possible with Achilles tendinitis and muscle injury of the gastrocnemius and plantar muscle. This test has been shown to be an "unreliable test for DVT." The test is done by using slow dorsiflexion of the foot, knee extension, or gentle squeezing/deep palpation of the affected calf to elicit deep calf pain because "in theory, the inflamed nerves in the veins within the muscle are compressed or stretched causing deep calf pain. One main reason this test is unreliable is that only "about half of all clients with DVT experience pain and Homan's sign" (Goodman and Snyder & O'Sullivan and Schmitz).
Reference
- Autar R. Nursing assessment of clients at risk of deep vein thrombosis(DVT): the Autar DVT scale. Journal of Advanced Nursing1996(23):763-70.
- Farris, James, DPT, PHD. Heick, John DPT, PHD. Screening for DVT’s with Clinical Guidelines, 2012 pathology lecture, Arizona School of Health Sciences
- Goodman, C. C., Teresa E. Kelly snyder. (2007). Differential Diagnosis for Physical Therapists Screening for Referral: Saunders Elsevier.
- O'Sullivan, S. B., Thomas J. Schmitz. (2007). Physical Rehabilitation (5th ed.): F.A. Davis Company.
- Riddle DL, Wells PS. Diagnosis of lower extremity deep vein thrombosis in outpatients. Physical Therapy. 2004 Aug;84(8):729-35.
- Siccama RN, Janssen KJ, Verheijden NA, Oudega R, Bax L, van Delden JJ, Moons KG. Systematic review: Diagnostic accuracy of clinical decision rules for venous thromboembolism in elderly. Ageing Res Rev. 2010 Dec 3.
- Wells PS, Hirsh J, Anderson DR, Lensing AWA; et al. Accuracy of clinical assessment of deep-vein thrombosis. The Lancet; May 27, 1995; 345. 1326-1330.
- Wells PS, et al. Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. N Engl J Med. 2003; 349(13):1227-35

{kind=link}